Meta description: Answers technical questions about pd measurement online, ipd accuracy try on, and how a link-based pupillary distance try on (tryitonme.com) delivers accurate, zero-code virtual try-on for eyewear — Book a demo.
This article explains pupillary distance try on and how accurate PD measurement online matters for lens centration, wearer comfort, and conversion in online eyewear sales. We’ll define PD vs IPD, compare measurement methods, review technical pitfalls, and show how modern virtual try-on (VTO) systems use multi-frame/AR approaches to improve ipd accuracy try on. Finally, you’ll get a practical validation checklist and a fast, zero-code option for merchants.
Where clinical implications are discussed, we refer to peer-reviewed material on PD and lens centration. For practical industry context on online PD techniques and business impact, see this industry analysis.
Definitions — binocular PD, monocular PDs, IPD, units (mm)
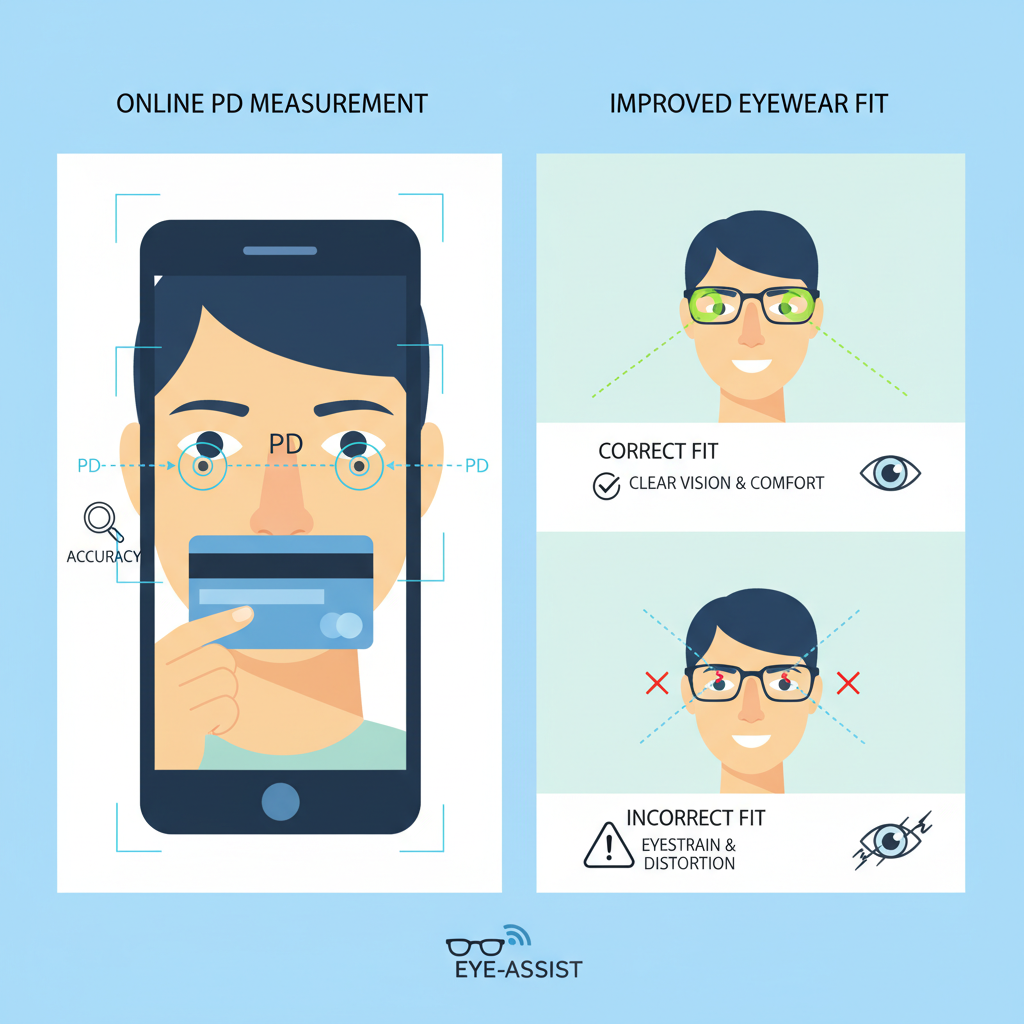
Accurate PD is required so the optical center of each lens aligns with the wearer’s visual axis; misalignment can induce prismatic effects, reduce visual acuity, and increase discomfort. See clinical discussion of how centration impacts visual function and optical effects: PMCID: PMC10389117. Practical takeaway: for prescription eyewear, PD errors matter — small millimeter offsets can change the optical experience.
How it works: user places a known-size object (credit card, reference card) next to their face; a single photo is used to scale pixel distances. Limitations include planarity assumptions, camera tilt, and distance errors. See practical discussion: industry analysis on accurate PD measurements.
Advantages: captures multiple frames, exploits small natural motion to resolve depth and pupil center, and can aggregate measurements to reduce noise. Clinical and technical context for multi-frame approaches: PMCID: PMC10389117 and the industry analysis.
Sources of variability
Each of these can create millimeter-level error; for example, a 10° yaw can produce several millimeters of apparent PD shift.
Single reference objects can fail if placed off-plane relative to the face or if the camera-to-face distance differs from assumption. Device variability (phone model, front vs rear camera) further complicates consistent scaling. See practical notes: industry analysis and mobile performance notes.
Distinguishing true IPD from apparent PD requires accounting for perspective and depth. Research and industry guidance indicate practical consumer targets; many systems aim for mean error near ±1–2 mm, with a high percentage of users falling within that band (see clinical review and industry analysis).
Modern VTOs use machine-learning landmark detectors to localize facial keypoints and estimate pupil centers robustly across lighting and skin tones. The clinical overview of landmarking approaches is discussed here: PMCID: PMC10389117. For an example VTO product context see: tryitonme eyewear virtual try-on.
Calibration strategies include explicit reference objects (cards) or intrinsic cues (average facial proportions and nose width). Cards provide scale but are sensitive to placement; intrinsic cues avoid extra props but rely on learned priors. Combining both as fallbacks improves robustness (see industry analysis).
Aggregating across multiple frames reduces transient errors. UX prompts — “look straight,” “remove glasses,” “rotate slowly” — produce better frames. Quality checks (confidence scores, required frame count) let the product decide when to accept a measurement or ask the user to retry. Aggregation benefits are discussed in the clinical literature: PMCID: PMC10389117.
Book a Demo at tryitonme.com.
High-level accuracy approach: tryitonme.com applies camera-native facial landmark detectors and pupil estimation, combines intrinsic cue calibration with optional reference-card scaling, and uses multi-frame aggregation and pose normalization to produce a stabilized PD reading. These approaches align with current clinical and industry practices: clinical review and industry analysis.
If automated confidence is low, the product supports manual PD entry as a fallback (merchant-configurable).
See the demo and merchant signup: tryitonme.com. Additional merchant context: blue light glasses try-on.
These UI patterns are widely used; specific implementations vary by merchant.
Clinical validation guidance: PMCID: PMC10389117 and industry testing context: industry analysis.
These metrics let product teams compare against acceptable thresholds and regulatory/clinical expectations. See clinical context: PMCID: PMC10389117.
Industry evidence for conversion/returns uplift is discussed here: industry analysis. Merchant-specific numbers available from tryitonme.com.
Copyable UI instructions (use verbatim in product flow):
Practical guidance is based on user best practices and clinical lighting/gaze guidance: industry analysis and clinical review.
Hypothetical merchant scenario (labelled hypothetical — no reliable source):
These are illustrative figures. Merchants can request real accuracy and KPI reports from tryitonme.com.
| Approach | Pros | Cons |
|---|---|---|
| Link-Based VTO (tryitonme.com) | Zero-code, fast to deploy, cross-channel, minimal engineering | Less customization than in-house SDK |
| SDK/API Integration | Deep customization, full control | Longer development, higher engineering cost |
For merchants prioritizing speed-to-market and reduced engineering overhead, link-based VTO is often the pragmatic choice. See related analysis: industry analysis.
Accurate pupillary distance try on is a practical, measurable way to improve fit, lower returns, and increase shopper confidence. Modern VTOs that combine landmark detection, multi-frame averaging, and solid UX guidance can reach consumer-grade accuracy suitable for many prescription lenses. If you want a turnkey, zero-code implementation, tryitonme.com delivers link-based PD try-on with fast onboarding (6‑month package workflow and try-on links delivered in under 3 business days). Visit tryitonme.com to view the demo, request a technical accuracy report, or Book a Demo.
Systems using multi-frame/AR approaches often report mean errors in the low millimeter range and target ±1–2 mm for consumer eyewear. Exact performance depends on device, lighting, and user compliance. See clinical context: PMCID: PMC10389117 and industry notes: industry analysis.
Yes for many consumer prescriptions when using validated, multi-frame systems and following best practices. For complex prescriptions or clinical concerns, recommend in-person verification.
PD is the pupillary distance between the eyes; IPD usually refers to the binocular PD. Monocular PDs are separate left/right measures from midline and are important for lens centration in progressive or asymmetric prescriptions.
Front-facing smartphones with good HDR and video capability are generally the most reliable in practice (recommendation; not a formal study).
Run a validation protocol: collect a diverse sample, record device mix, compare vendor PD to clinical pupilometer readings, and report mean error, % within ±1/2/3 mm, standard deviation, and failure rate. Clinical guidance: PMCID: PMC10389117.